Do you plan beyond the extraction?

Joe McEnhill addresses the short and long-term factors that you should consider after extraction of the tooth.
As dentists, whilst we are performing extractions day in and day out, we’re sometimes guilty of not always considering the bigger picture and what happens post-extraction. Extractions are not usually the completed plan, the fait accompli, and so it is always prudent, and advantageous to plan ahead and think about how we can make our patients’ life better and not inadvertently make it worse.
It’s never our intention to traumatically remove a tooth, but sometimes it is inevitable. Essential to this is levelling up our extraction skills to be able to successfully and quickly remove the tooth whilst ensuring the patient has an easy recovery.
First and foremost, whenever we’re removing a tooth, we must understand how the failing tooth can affect the alveolar bone and how it subsequently affects the restoration of the gap, as well as assess the urgency of the situation. Once the extraction has been performed, patients aren’t always happy being left with gaps in their mouth so we must think of the bigger picture and how we are going to manage the patient next.
For example, we should ensure there is as much residual bone/soft tissue left as possible. It is also best to leave our options open and give our patients the choice of opting for immediate implants, possibly with immediate loading. If, however that’s not going to be the case, it then raises the question as to whether we should graft the socket and the soft tissue. I am always thinking about a one surgery approach, but there are times that we can use the biology of healing to our advantage. Thinking of those thin gingival biotypes and the gains in soft tissue we get just by the socket healing over is an easy win.
Classifying the alveolar process
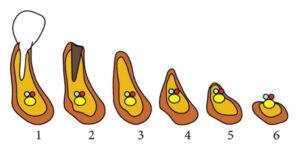
graph 1
It’s important to understand that six months post-extraction, the anterior zone can lose up to 4.5mm, in both the horizontal and vertical bone. This tends to be towards the higher end of the spectrum with those who have thin buccal plates – of which 2 out of 3 people have. [I]
The Cawood and Howell classification system of changes in shape of the alveolar processes shows the pattern of resorption and thus enables clinicians to anticipate and avert future problems [II]. (Graph 1)
When considering how to move onto the next treatment modality we ideally want our patient to have a substantial amount of bone (classification 1 and 2). It’s not just about getting the tooth out, but how can we prevent the pathway where the patient is losing bone and heading into classification 4, 5 and 6. This really matters even if the patient is not going for an implant. Even the humble denture stands a better chance when the ridge is well formed!
Creating less trauma for the patient
The goal remains to achieve a one surgery approach whilst ensuring the patient goes through less trauma and surgery. With an array of causes for tooth failure, it’s important to consider anything that can cause acute or rapid bone loss. Below are 3 case examples and the considerations when timing the extraction.
1. Carious roots:
We have all seen those patients that have dark brown/black carious roots down to gum level. Incredibly these roots rarely cause any real symptoms and may persist for years without any problem. You could easily argue that they should be removed, however they are often serving us by preventing bone and soft tissue loss. I will usually only remove these just when I’m ready to place an implant.
2. Chronic infection:
Peri-apical pathologies can be slow moving and often are incidental findings. You will need to assess the amount of damage to the bone. If there is an intention to remove the tooth to place an implant, can it be done simultaneously? Any further damage is likely to be slow moving, so there is the opportunity to be strategic in the timing of our extraction.
3. Root fracture:
Sub-crestal oblique or vertical root fractures can cause a lot of bone damage rapidly and I consider these to be urgent if I want to maintain bone. There is nothing to be gained by keeping these, they should be removed immediately or referred to the implantologist with a degree of urgency. Regrettably even then it’s often too late.

Image 1- bone damage from root fracture

Image 2 - bone damage from root fracture

Image 3 - physiological bone resorption, this shows how even broken and carious roots can maintain bone dimensions

Image 4 - physiological bone resorption, this shows how even broken and carious roots can maintain bone

Image 5 - socket shield in place
Instrumentation process
There is an array of instruments available, and we all have our “go to’s”, but I generally tend to use the following instrumentation process for extractions.
Starting with the elevators, my 2 & 3mm luxators are the workhorses which begin to disrupt the periodontal ligament and dilate the socket. Forceps should be chosen so they fit well, and when in use, you should see a progressive increase in tooth mobility. However, every one of us knows that the pressure and rotation applied doesn’t always result in a successful extraction; knowing when to stop is key so as not to break the root or buccal wall. It is a common pitfall to hit a stumbling point but to carry on and apply more and more pressure, something is going to break. We need to stop and reassess; we need to pivot. We need to make the socket larger or the tooth smaller, or both.
Take for example, an extraction of an upper first premolar or molars, in this situation I would commonly turn to the next workhorse of my armamentarium, the fast handpiece. I will separate the roots, whilst taking care not to damage the adjacent teeth. This can ensure a much easier delivery whilst helping preserve the bony walls. My advice, make your extractions a single root – it is simpler and more predictable to turn molar teeth into single roots. If we create space between the roots, they now have room to concertina in towards each other and away from the bony walls thus preserving the integrity of the socket.
Atraumatic extraction – what next?
As referred to earlier, our primary goals are to achieve everything in “one surgery” or at the very least prevent physiological bone resorption. Our options post extraction will centre around five areas: connective tissue graft, ridge preservation, ridge augmentation or immediate implants, with or without immediate loading. Another popular approach to consider in implant placement is Partial Extraction Therapy (PET), which involves the sectioning and removal of the crown of the non-restorable tooth, leaving only the root, which is then sectioned into two parts mesiodistally [III].
In terms of material selection, autogenous bone is often considered the gold standard in implant dentistry, providing a proven and predictable method for ridge augmentation and defect repair for dental implant placement. However, there are alternatives to consider such as allograft (human donor), xenograft (bovine, equine and porcine) and alloplast (synthetic). Knowing which material to choose will be based on understanding several factors such as the resorption time, ridge morphology, and whether it’s an immediate or delayed implantation.
To conclude
In summary, it is important to note that fractured roots are an urgency. The GDP is the first responder to a failing tooth and the quicker the patient is seen, the better. The early decisions made around the tooth extraction will send your patient on a difficult pathway or one with less trauma and a reduction in overall treatment time. This will result in an increase in patient acceptance, along with a psychological benefit.
Elevating yourself to the next level and learning more skills, whether it’s getting better at surgical extractions or socket shielding, can lift your game and ultimately help increase your own satisfaction levels, improve your patient’s treatment journey and most likely increase profitability.
Watch the full webinar ‘Planning beyond the extraction’ here or to find out more about how Joe McEnhill can help you with basic oral surgery and extractions visit our chairside visitation service here.
Article feedback
Article Author
Joe’s 20+ years’ dental experience includes; working in Oral Maxillo-facial in major reconstructive surgery, completing extensive training in hard and soft tissue grafting, full mouth rehabilitations and digital smile design. Joe also runs an oral surgery course Northern Ireland and mentors dentists in oral surgery and dental implants. He is the current regional representative for the Association of Dental Implantology.





