Aesthetic Ridge Preservation

Imi Nasser demonstrates the power of ridge preservation during orthodontic treatment.
This patient presented with orthodontic crowding and a dislike for her enlarged crown on UL1 and “higher gum line.” She requested teeth straightening and an improvement in the gum line on this crown.
Following the clinical & radiographic examinations, it was identified that the UL1 was restored with a post-retained crown and suffering with internal resorption. It also highlighted that the alveolar ridge was extremely narrow.
Treatment options.
The treating orthodontist advised that the UL1 should be removed prior to orthodontic treatment and the replacement options were discussed with the patient who preferred an implant retained restoration. The concern remained that whilst upper and lower orthodontics were being carried out, there would be vast hard & soft tissue resorption rendering implant treatment to require complex, staged procedures in due course.
Treatment plan.
It was thus decided to carry out a ridge preservation graft to retain the existing alveolar ridge width and to use an open healing concept to encourage new soft tissue growth, increase keratinised tissue and avoid distortion of the mucogingival junction. This was carried out using the combination of MinerOss® Blend Allograft and a dense PTFE membrane.

1 - pre op
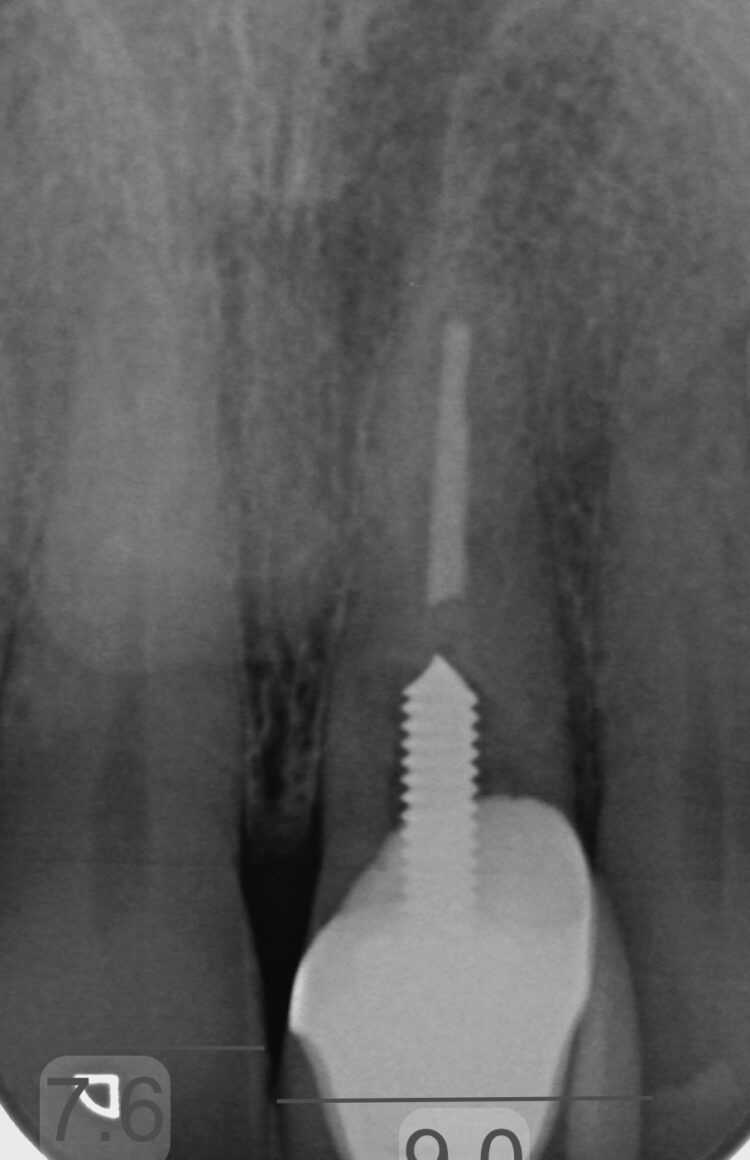
2- pre op rad
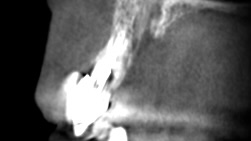
3- CBCT
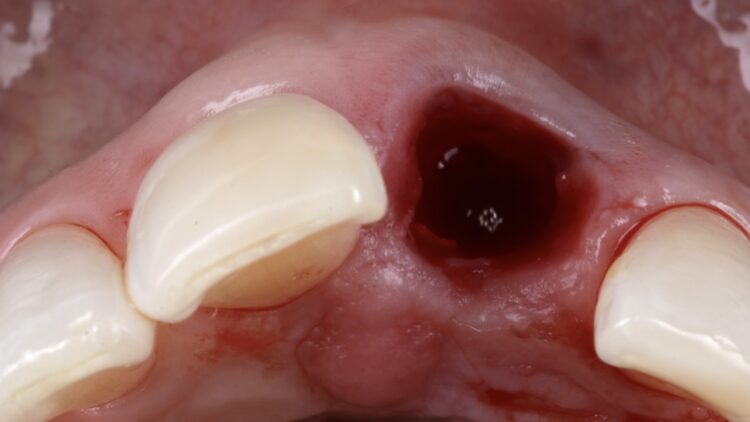
4- extraction

5- graft placement
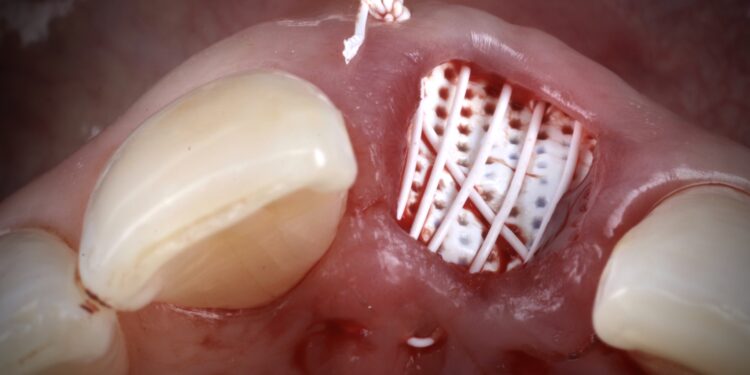
6- membrane stabilisation

7- 4 weeks healing

8- post ortho

9- implant placement
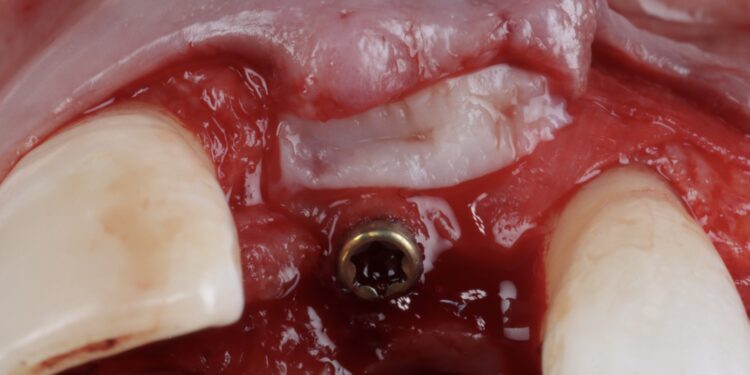
10- GBR & CTG
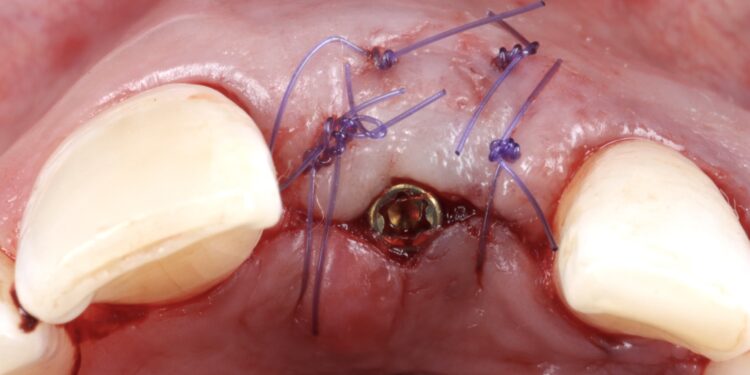
11- sutured shot

12- healed shot

13- healed shot

14- healed shot

15- emergence

16- final shot
Implant phase.
Once the orthodontic treatment was completed, the site was re-evaluated, and it was clear to see that the gingival zenith had significantly improved. The patient was advised that without re-contouring the mesial aspect of the contralateral central incisor there would be a midline black triangle. She rejected the option of composite addition to alter the triangular shape of the UR1 and thus we proceeded to complete the treatment without this. The implant was placed with simultaneous buccal GBR & connective tissue graft following a transmucosal approach. Following a healing period of 4 months, the restorative treatment was initiated with a temporary crown to develop the emergence profile. Once the gingival zeniths had been matched, the patient was delivered a permanent screw retained crown.
Conclusion.
This case demonstrates the power of ridge preservation whereby significant hard tissue grafting was avoided entirely in a patient with an extremely thin maxillary alveolus. The improvement in soft tissue contours is evident to be seen even with a healing period of 18 months post extraction with excellent keratinised tissue volume and no distortion in the mucogingival junction.
To find out more about ridge preservation click here or to attend a course on Ridge Preservation with Imi Nasser click here.
Article feedback
Article Author
BDS (Bris); MFDS RCS (Edin) MSc Implantology (Bris). Dr Imran Nasser qualified in 2006 from Bristol University and then completed hospital posts in Oral & Maxillofacial Surgery. He completed his Master of the Faculty of Dental Surgery in 2009 and his Master’s degree in Implantology in 2010-2014. For the past four years in succession (2021-2024), Imi has received the accolade of winning the UK Aesthetic Dentistry Awards in Implant & Ceramic categories. Imi is Practice Owner of Cheltenham & Cotswold Dental (formed in 2020). His practice is predominantly referral based; and limited to soft tissue surgery, bone grafting, sinus grafting, ridge preservation, implants & aesthetic restorative cases. He is passionate about sharing his experience and runs various training courses for colleagues.





