Immediately loading an anterior implant with occlusal considerations

Dr Imran Nasser presents a recent case and offers advice on how to mitigate the potential challenges that can arise from immediately loading an anterior tooth.
Introduction
Immediate implant protocols have been proven safe and effective in a number of clinical scenarios. For optimal outcomes, clinicians must take precautions to mitigate potential complications with each case they treat. Occlusal considerations must be included in the assessment and planning phases of treatment, for example, to determine the implant’s ability to withstand the forces it will be placed under if loaded immediately. The literature suggests no significant difference in success of non-occlusal and occlusal modalities of implant loading,[i] when case selection and techniques are sound.
The following case demonstrates how implant placement alongside a deep overbite may be effectively managed.
Case presentation
A female patient in her mid-50s was referred due to pain around the gingival margin of the UR1. The tooth had previously been root filled and crowned, and was now unrestorable. External root resorption was confirmed with a periapical radiograph, which showed that the distal bone peak was absent. Located in the aesthetic zone, the missing distal peak meant that the remaining papilla would disappear after the tooth was extracted, and thus needed addressing to avoid the formation of a black triangle.
Assessment and planning
The comprehensive assessment revealed tight interocclusal space and an increased overbite. The occlusion could present a risk of complications alongside immediate loading protocols, but the implant chosen offers excellent primary stability and confidence that it can withstand the loading forces, eliminating any concerns. The author would not have the same level of confidence with previous implant systems he has used.
A CBCT scan was taken, using cotton rolls to keep the teeth separated during image capture for maximum accuracy and seamless digital integration with the intraoral scan. This was used to evaluate the volume of apical and palatal bone available to stabilise an immediately loaded implant, and to determine the appropriate implant size for a jump gap of at least 3mm. The buccal plate thickness was also assessed – improved outcomes and reduced resorption are achieved when this is at least 1mm. For optimal success with immediacy, the implant should be placed 1mm below the buccal plate, 4mm below the level of the proposed CEJ of the final tooth, and palatally positioned.

Figure 1: Initial presentation upon referral

Figure 2: Pre-operative radiograph
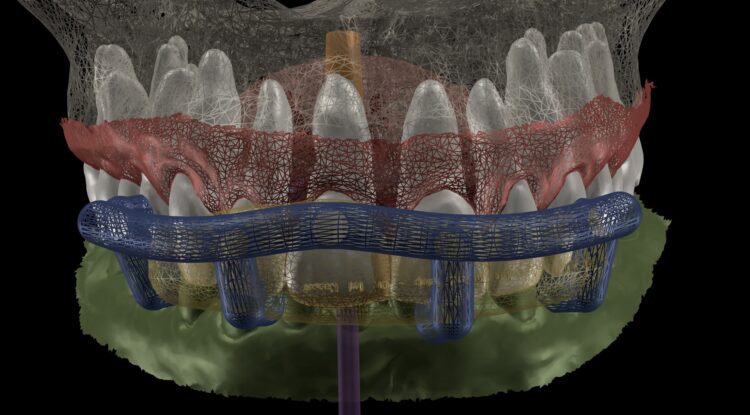
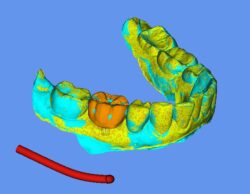
Figure 3: Digital planning for surgical guide

Figure 4: SMOP guide featuring 3.8mm implant sleeve included

Figure 5: Verification jig if original crown were to be used
An intraoral scan was taken, including the entire palate to provide a precise reference for the CBCT scan. This enabled the accurate merging of the intraoral and CBCT scans to create a diagnostic wax-up for the provisional restoration.
Smile Cloud software with AI-driven smile design features was used to assist treatment planning and provide short animations for use in patient communication. The same data was put into SMOP software to design the surgical guide, which is essential to optimise primary stability for immediate loading.
Two temporaries were requested from the laboratory. One was fabricated from the SMOP guide affording high visualisation to increase precision of fit. The second temporary had a stent that sat over the incisal edges, which could be used to confirm accurate positioning.
Implant placement
On the day of surgery, the post crown was removed, and the tooth sectioned to ease extraction while preserving the buccal plate. Forceps were used to deliver the fragments, with extensions to simplify pick-up (Hu-Friedy). The granulation tissue was removed using a Lucas curette.
The surgical guide was checked in the mouth, ensuring it was fully seating and not in contact with the adjacent teeth.

Figure 6: Post crown removed, distal resorption visualised, and root sectioned

Figure 7: Forceps used to remove fragments

Figure 8: Granulation tissue removed

Figure 9: Surgical guide fit check to ensure accurate seating

Figure 10: CONELOG 3.8mm implant placed through guide
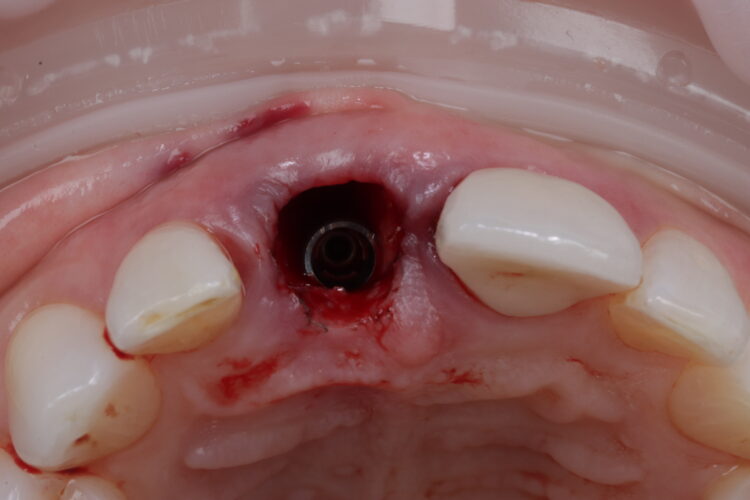
Figure 11: Implant placed in close contact to palatal bone with jump gap visible
The standard CONELOG® (BioHorizons Camlog) guided drill sequence was followed. The Guided Surgical Kit is very simple to use with a streamlined number of drills. The CONELOG® drills support primary stability, with side-cutting features and apical threads that engage the native bone.
The CONELOG® Progressive-line implant maximised primary stability and in this case the implant was inserted at 70Ncm. The pre-made temporary was used as the temporary restoration; however, there would also be the option of modifying the existing crown.
The implant was placed in close contact with the palatal bone, 1mm below the buccal bone height. A temporary cylinder abutment was connected, with flowable composite placed to attach the temporary restoration. The composite resin was used to create the optimal emergence profile ensuring a highly polished restoration in the transition zone.
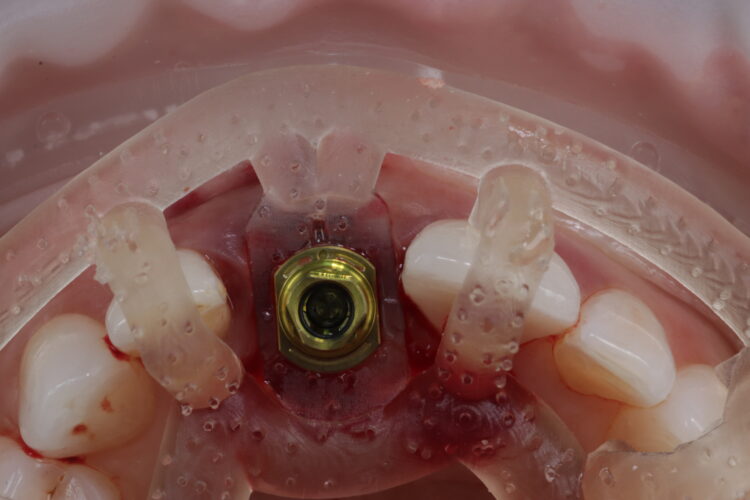
Figure 12: Implant delivered fully guided

Figure 13: Temporary restoration created prior to grafting to ensure material is not contaminated with composite
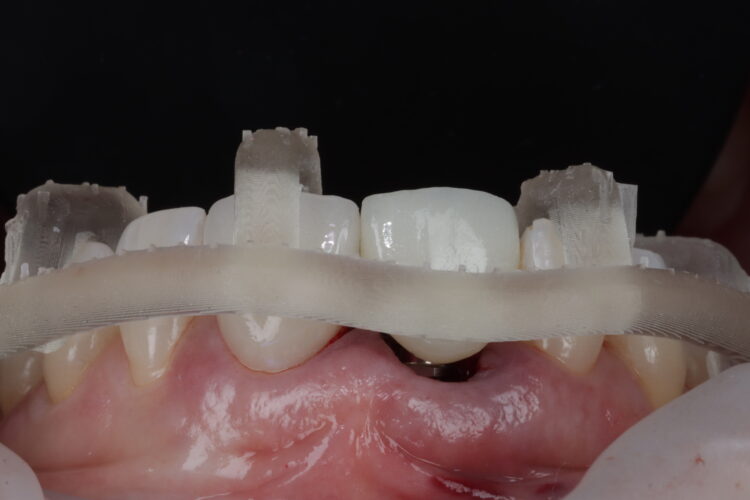
Figure 14a: Lab temporary tried in with SMOP verification

Figure 14b: Second guide tried in mouth, demonstrating the accuracy of impant placement with regards to planning

Figure 15: Flowable composite attaching temporary to abutment
Soft tissue regeneration
A free gingival graft was harvested from the palate, allowing enough tissue to reach between the base of each papilla and this was de-epithelialised to obtain the connective tissue. A thickness of 1mm is adequate, but in this instance, it was made intentionally thicker at the disto-buccal aspect to help plump up the papilla where bone loss was greater. The connective graft tissue was stabilised with three resorbable sutures placed, positioning the connective tissue graft 1mm below the free gingival margin.
A bone graft was then performed, adding MinerOss® Blend (BioHorizons Camlog) to the jump gap. This affords an ideal combination of cortical and cancellous bone, delivering high bone density and reliable revascularisation to ensure the fast and predictable turnover of bone.
The temporary restoration was then reintroduced and the surgical site closed tension-free. Vertical sling sutures were placed through both papillary areas over the contact points to hold the tissue up, create a prosthetic sealand to combat natural shrinkage.
A post-operative radiograph was taken to confirm that the crestal bone was not compressed and there was no convexity in the area to allow space for the soft tissue graft to expand, proliferate and grow.
Upon review eight weeks later, healing had been uneventful. The temporary restoration will be left in place for six months to allow the tissues to mature prior to final restoration.

Figure 16: CTG placed from papilla to papilla

Figure 17: CTG stabilised from papilla to papilla
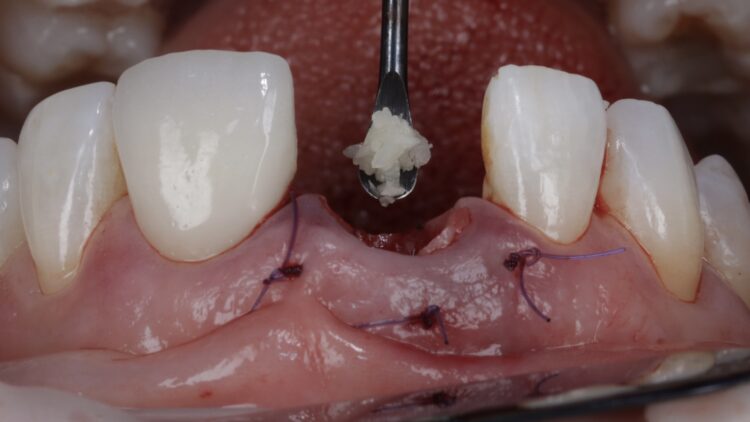
Figure 18: MinerOss Blend added to jump gap
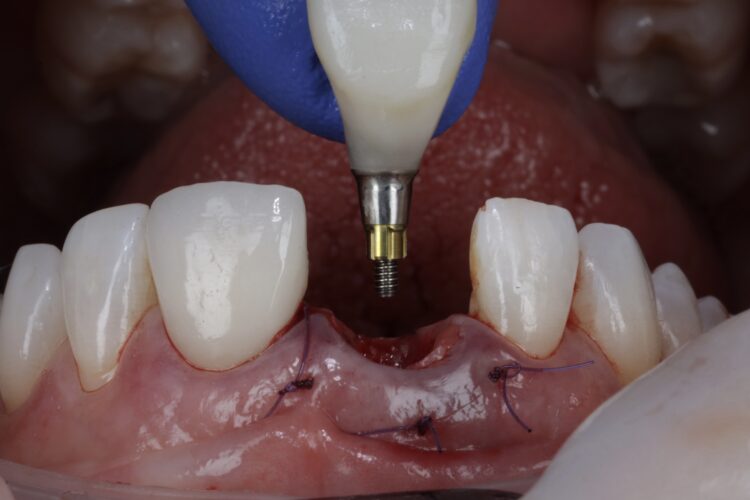
Figure 19: Temporary restoration try in

Figure 20: Site is closed with vertical sling suture, placing the soft tissue in close approximation to the subgingival profile of the restoration
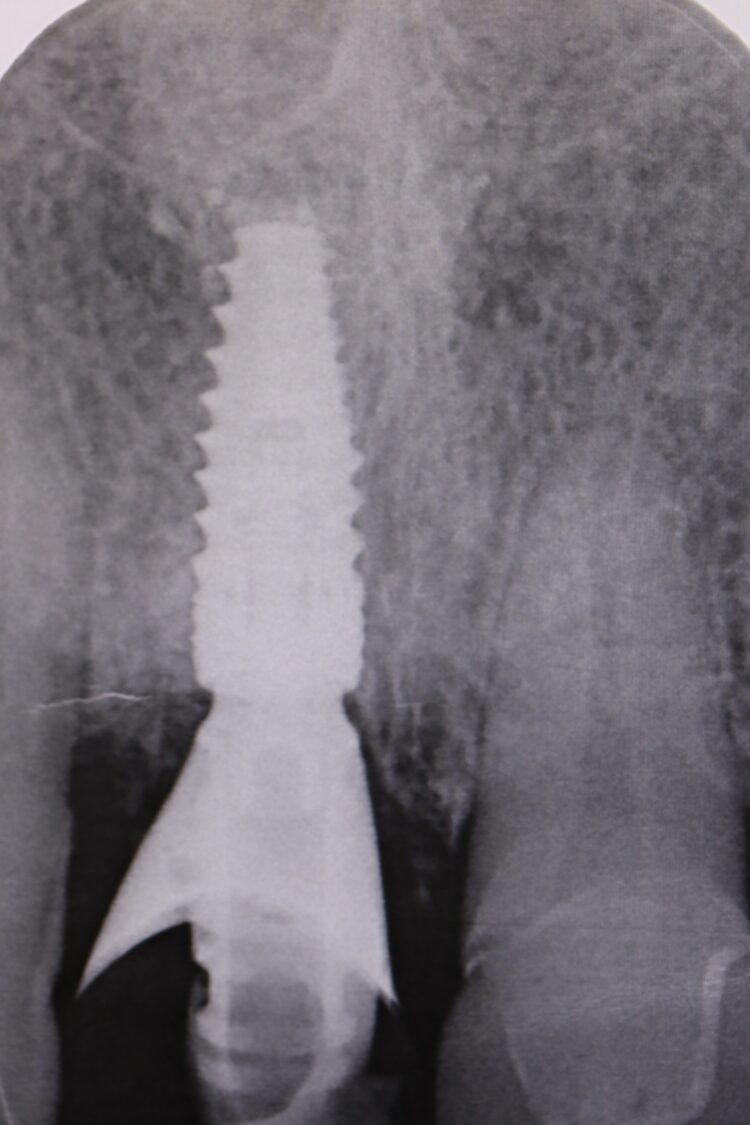
Figure 21: Post-operative radiograph without compressing crestal bone

Figure 22: Eight week post-operative review
Reflections
A key factor in this case was the patient’s occlusion. The deep overbite made immediate loading a higher risk, so a guided workflow was crucial to ensure primary stability was not lost. Occlusion, parafunction and bruxism are all critical factors when assessing for implant placement, especially alongside immediate loading.
The CONELOG® implant system is my go-to for immediate cases, particularly where strength and function must be balanced with aesthetics. Its long conus reduces micromovements and it affords greater positional stability than other conical systems I have used. The 3.8mm diameter is the ideal combination of surgical strength and aesthetic considerations. The Guided Surgical Kit is simple to use and has a streamlined workflow for increased efficiency.
To discuss how you can implement the Conelog Progressive-Line into your implant practice, contact our team.
For all your implant educational needs, visit our dedicated education website, where you can find a range of courses to suit you.
Article feedback
Article Author
BDS (Bris); MFDS RCS (Edin) MSc Implantology (Bris). Dr Imran Nasser qualified in 2006 from Bristol University and then completed hospital posts in Oral & Maxillofacial Surgery. He completed his Master of the Faculty of Dental Surgery in 2009 and his Master’s degree in Implantology in 2010-2014. For the past four years in succession (2021-2024), Imi has received the accolade of winning the UK Aesthetic Dentistry Awards in Implant & Ceramic categories. Imi is Practice Owner of Cheltenham & Cotswold Dental (formed in 2020). His practice is predominantly referral based; and limited to soft tissue surgery, bone grafting, sinus grafting, ridge preservation, implants & aesthetic restorative cases. He is passionate about sharing his experience and runs various training courses for colleagues.