Restoring quality of life with full arch reconstruction
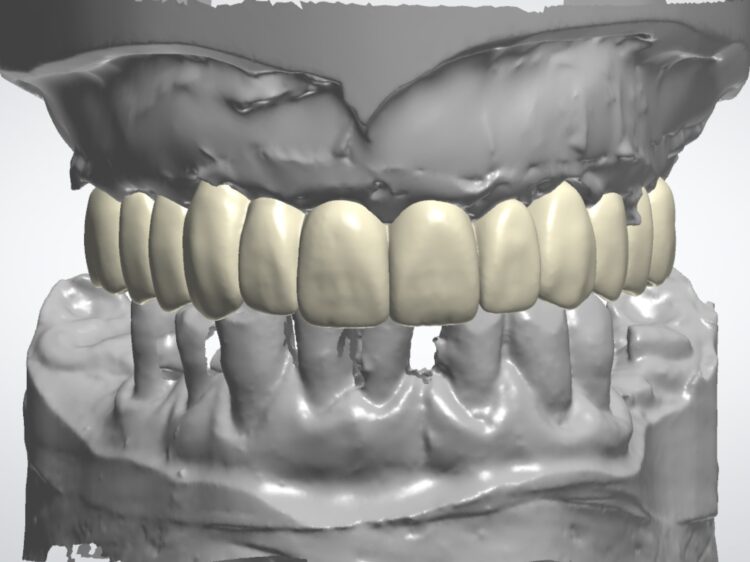
Figure 21a: Digital smile design of the final prosthesis
Dr Nikolas Vourakis presents a complex full arch case, using a guided surgical approach to optimise surgical and prosthetic accuracy.
A 60-year-old male patient presented with major concerns about unsatisfactory smile appearance, limited masticatory function and pain while chewing. The patient was in good general health. The clinical and radiographic examination revealed failing ceramic restorations, rampant caries, non-restorable teeth, soft tissue inflammation, residual roots and missing teeth. Comprehensive digital records, including extraoral and intraoral clinical photographs, were collected as part of the initial assessment. The case was deemed suitable for full arch implant-retained restoration using advanced techniques.
Treatment planning
As in all cases, the patient was presented with all options and their related benefits, risks and limitations. These included no treatment, extraction of the remaining teeth and fitting of a removable denture, or extraction with an implant-retained full arch prosthesis.
The latter was the professional recommendation and the patient’s preferred option, despite it presenting the most advanced procedure. Full arch reconstruction is always a complex treatment solution, but it can substantially increase many patients’ quality of life. Comprehensive treatment planning is crucial to mitigate the risks and minimise the chance of complications for the smoothest patient experience and most predictable clinical results.
Full arch reconstruction is always a complex treatment solution, but it can substantially increase many patients’ quality of life.
Some of the most common complications include biological issues due to implant malposition like peri-implantitis [i] or mechanical/prosthetic problems such as fracture of the provisional and the final prosthesis.[ii] Computer guided implant surgery can be valuable for ensuring implants are placed in an ideal position during full arch rehabilitation, allowing a soft tissue emergence with a natural-looking FP1 fixed dental prosthesis (FDP).[iii] [iv]

Figure 1: Initial situation frontal view

Figure 2: Left lateral view at presentation

Figure 3: Right lateral view at presentation
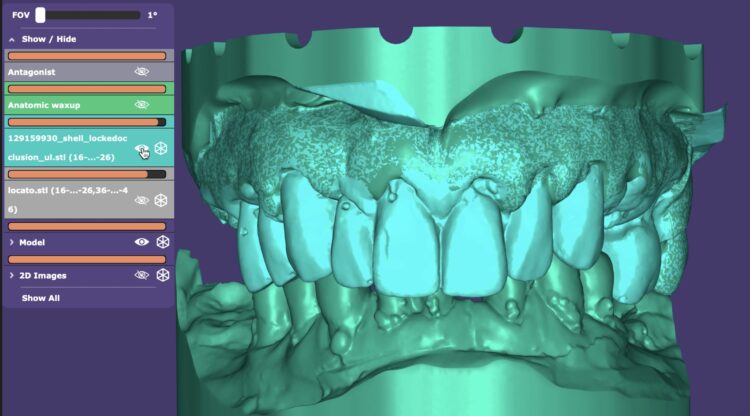
Figure 4a: Digital planning initial situation

Figure 4b: Digital extraction of teeth
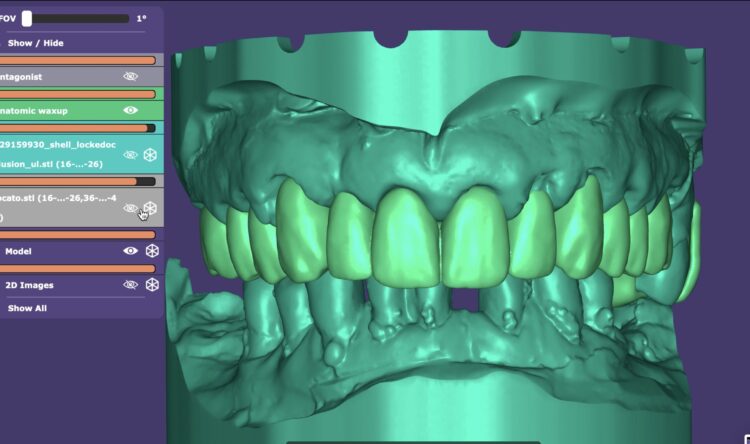
Figure 4c: Exocad digital smile design

Figure 4d: Digital design of provisional restoration
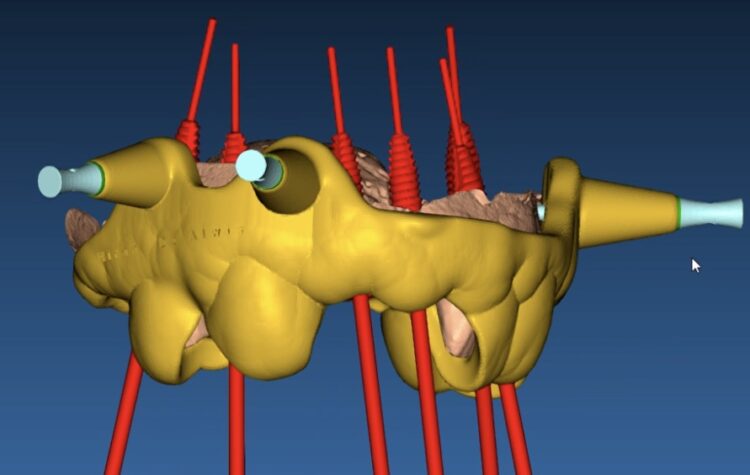
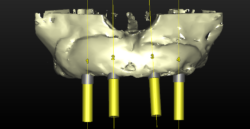
Figure 5: Teeth and bone supported surgical guide planning for accurate implant placement
Ensuring the clinician is prepared for these risks, and they have been adequately communicated with the patient, treatment can be highly successful with diligent planning and patient compliance with excellent oral hygiene. This patient underwent extensive courses of hygiene to improve the health of the periodontal tissues and was motivated to improve his cleaning routine.
When ready, the surgical planning involved a fully digital, prosthetically-driven workflow, with full dentist and dental technician collaboration. Intraoral scans (IOS) were merged with the DICOM data from the CBCT to optimise data capture and facilitate an accurate digital plan for implant placement and prosthesis design. The digital files and photographs were imported into a Digital Design Software (EXOCAD) and a personalised, facially-driven tooth library was used to perform an initial virtual wax-up.

Figure 6: 3D printed composite provisional prosthesis with palatal support

Figure 7: Surgical guide
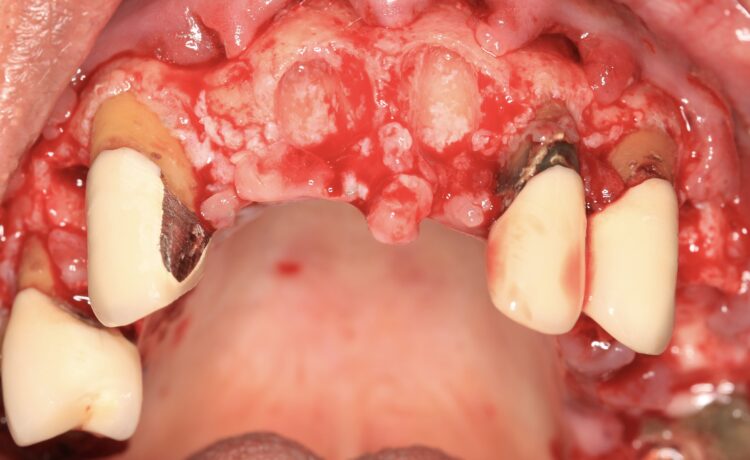
Figure 8: Remaining teeth to support surgical guide

Figure 9: Teeth supported surgical guide secured with anchor pins

Figure 10: Implants placed through surgical guide

Figure 11: Provisional restoration located in the mouth using the hard palate
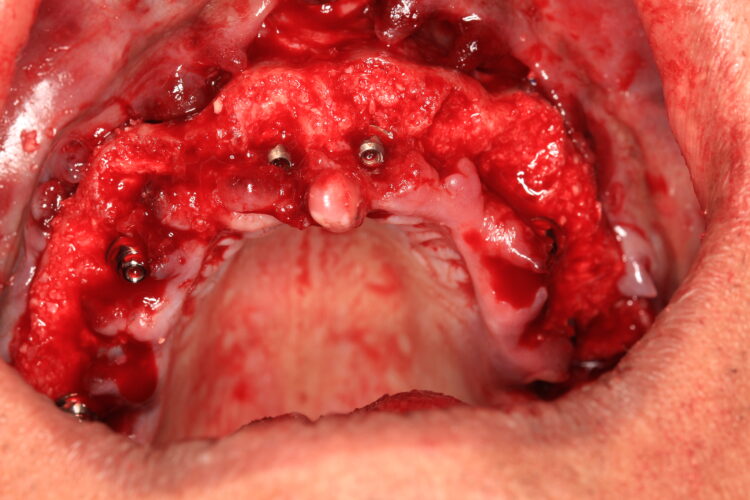
Figure 12: Allograft in the sockets and around the implants
The use of a surgical guide for the accurate and precise placement of the dental implants was chosen in this case. The positions and angulations of the implants were planned according to the ideal virtual wax-up that was produced. We decided to create a tooth-supported acrylic guide for fully guided surgery, supplemented by bone-fixed anchor pins for enhanced stability. The most appropriate teeth for this were identified during this planning phase.
Surgical treatment delivery
The plan was followed meticulously on the day of surgery. The canines, left and right premolars and a right molar were used to support the surgical guide together with three bone anchor pins. Following the digital plan, all other teeth were extracted and thorough degranulation of the sockets was performed. No bone reduction was performed for both the provisional and final prosthesis in accordance with the Misch classification for an FP1 approach.[iv]
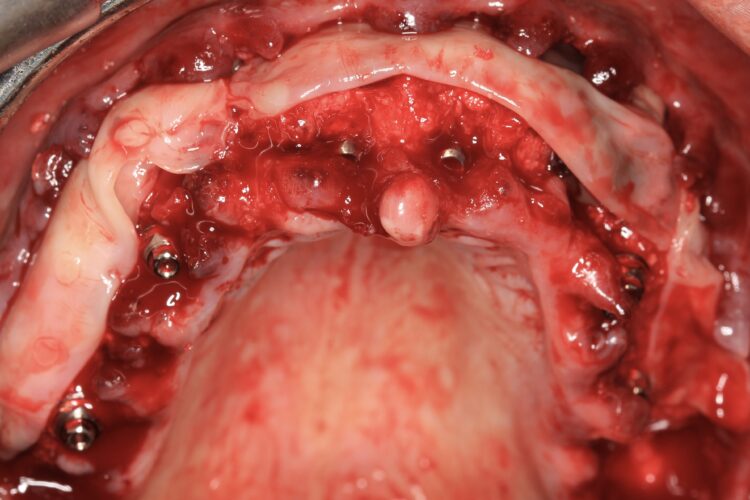
Figure 13: L-Prf for improved healing and soft tissue quality

Figure 14a: Provisional restoration Ovate Pontics design

Figure 14b: Provisional restoration Re-enforced with bended titanium wire

Figure 15: Provisional restoration in situ

Figure 16: Coronal advancement of the buccal flap

Figure 17: OPG of the provisional restoration in situ

Figure 18: Healing after two weeks
The implant beds were then prepared with the surgical guide in situ. Six CONELOG® Progressive-Line implants from BioHorizons Camlog were placed in accordance with the predetermined positions, depths and angulations. These implants were selected for this case because they feature an optimal thread design and tapered figure, promoting high primary stability – which is essential in full arch reconstruction cases.
The implants were placed through the guide for better accuracy and precision. A surgical primary stability of >35Ncm was achieved for each implant. Once the implants were placed, the surgical guide was removed, and the extraction of the remaining teeth was completed.
These implants were selected for this case because they feature an optimal thread design and tapered figure, promoting high primary stability – which is essential in full arch reconstruction cases.
In preparation for the provisional prosthesis, straight multi-unit abutments were fitted onto the implants and torqued to 25Ncm, followed by titanium cylinders. For the anterior implants in the areas of the central incisors, the Comfour Straight bar abutments were used. The narrow prosthetic platform of these Comfour abutments (4.3mm) compared to the wider prosthetic platform of the standard multi-unit abutments is advantageous as it provides more space for soft tissue thickness and stability of the therapeutic outcome in the long-run.
The design of the provisional prosthesis followed the Gallucci prosthetic guide protocol[i] providing a 3D printed composite bridge with palatal support. The palatal support sits below the fitting surface of the bridge and is only used to locate the bridge in centric occlusion using the hard palate of the patient. This bridge is an exact copy of the digital wax-up used to plan the implant positions. The use of guided surgery guarantees that the implants are placed precisely according to the plan.
The provisional restoration in this case had prefabricated prosthetic channels to match the same planned implant positions and angulations. This provisional was located in the mouth using the hard palate and attached on the titanium cylinders that penetrate through the bridge, with the use of a composite based light cured material.

Figure 19: Healing after three months

Figure 20: Soft tissue sculpturing during digital impressions
Figure 21a: Digital smile design of the final prosthesis
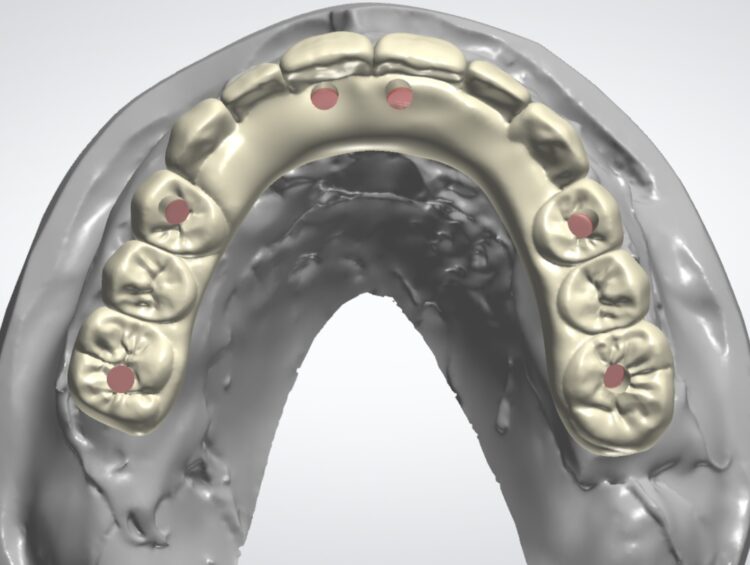
Figure 21b: Final prosthesis digital design occlusal view
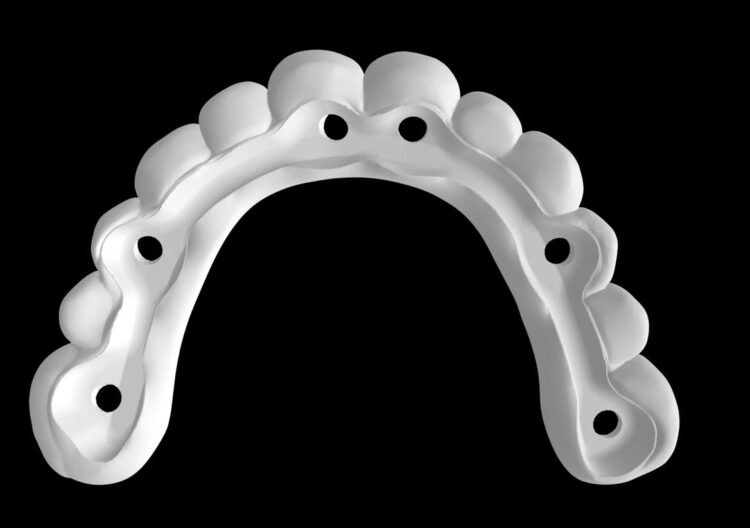
Figure 21d: Zirconia superstructure digital design

Figure 22a: Final zirconia titanium supported Fp1 prosthesis

Figure 22b: Final zirconia titanium-supported FP1 prosthesis
The provisional prosthesis was then modified; the palatal part was removed and the bridge was relined with the use of a composite based flowable material, making sure that mechanically polished deep ovate pontics were designed for adequate sculpturing and adaptation of the soft tissue. A titanium wire 2mm in diameter was inserted into the bridge improving its rigidity and strength.
A full thickness flap was reflected buccally up to the mucogingival junction followed by a split thickness flap with periosteal relieving incisions. Bone grafting materials were inserted into the sockets following socket preservation techniques. We used Mineralized Bone Allograft (MinerOss® by BioHorizons) mixed with autogenous bone particles collected during the drilling protocol, both inside the sockets and around the dental implants to fill the jumping gaps to the residual bone. Six 10ml tubes of blood were collected and L-PRF membranes were placed buccally to improve soft tissue healing and quality.
We used Mineralized Bone Allograft (MinerOss® by BioHorizons) mixed with autogenous bone particles collected during the drilling protocol
The finished and polished provisional restoration was screwed on the multiunit abutments at 15Ncm. The buccal flap was coronally advanced and closed with sling sutures using resorbable monofilament Glycolon 5/0 sutures.
This phase of treatment concluded with radiographs to confirm accurate implant placement. The patient was also given standard post-operative oral hygiene and care instructions. He reported no complications or concerns during the review appointment a week later.
Final restoration
After four months, an IOS impression was executed and a digital dataset created superimposing the soft tissue, implant scan bodies, antagonist and temporary prosthesis scanning files. To avoid any inaccuracy in scalloped interface reproduction due to quick collapse of the gingival tissue, the provisional prosthesis was scanned both intraorally and extraorally, capturing its overall contour and, in particular, the transmucosal surface at the pontic sites and emerging profiles.
A titanium substructure was digitally designed (Bridge Base by Atlantis) taking into consideration the functional and aesthetic virtual wax-up and emergence profile as the FP1 provisional prosthesis shaped it. This metal substructure was anatomically shaped at the gingival and occlusal sides in order to tightly adhere at the soft tissue interface leaving at least 2mm of clearance for the zirconia superstructure.

Figure 23a: Final restoration in situ

Figure 23b: Final restoration side views

Figure 24: Final prosthesis OPG

Figure 25: Final prosthesis one year follow-up

Figure 25b: Final restoration side views one year follow-up
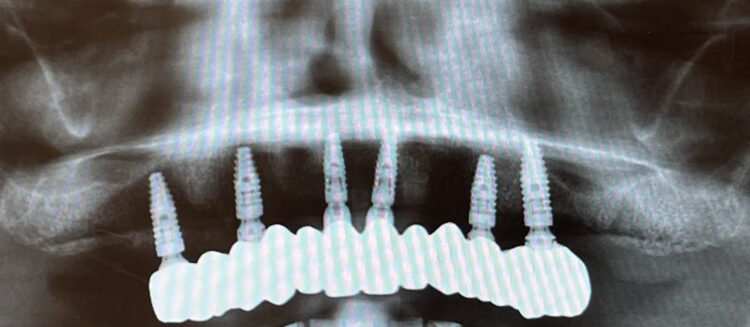
Figure 26: OPG one year follow-up
Based on the digital design and copying the approved provisional prosthesis, a zirconia overlay was milled. The overlaying zirconia superstructure was digitally designed to fit the metal substructure, accomplish a flawless finish line, avoid any undercuts and verify the path of insertion, thus facilitating the bonding procedures. The zirconia superstructure was bonded with the titanium substructure using a self-curing luting composite. The final polished screw-retained prosthesis was delivered and torqued to 30Ncm and the radiographic assessment was executed.
After the follow up appointments at one and four weeks, the patient was scheduled for periodic maintenance every three months. The retrievability of the final screw-retained zirconia-titanium supported prosthesis allowed management of the interface over time. At the one-year review, further growth and maturation of the soft tissue as well as the health of the keratinised peri-implant tissues were evident, without signs of bleeding on probing.
Outcome and reflections
The patient was thrilled with the final outcomes achieved in this case, as was I. The failing dentition was replaced by a fixed, long-term – with patient oral hygiene compliance – and cleansable solution, which will restore the patient’s quality of life.
Particularly in FP1 cases where a correct emergence profile has to be formed through the implant-supported immediate temporary prosthesis, a digital treatment plan and guided surgery offer a comprehensive workflow to achieve predictable high-end prosthetic results that mimic the natural dentition.
The translucent zirconia supported by titanium framework fulfils the aesthetic and mechanical requirements of an FP1 full arch prosthesis, while minimising the risk of fracture by providing a rigid yet passive joint to support the implants.[vi] The zirconia and titanium transmucosal surface characteristics (otherwise known as biocompatibility) create a highly polished interface for high cell adhesion and optimised gingival architecture.
The implant system chosen is just as important for full arch cases. It is crucial to work with products that will support both functional and aesthetic outcomes, while helping the clinician to minimise potential complications associated with this type of treatment.
Dr Nikolas Vourakis teaches for BioHorizons Camlog and is part of the Chairside Visitation programme. For more information please visit education.theimplanthub.com
Article feedback
Related Articles
- Implant replacement of the upper right lateral incisor utilising MinerOss and a connective tissue graft: a case study
- Maxillary bilateral sinus lifts with augmentation using allograft grafting material
- The delivery of ridge preservation treatment in preparation for future restoration with dental implants